
An AI algorithm trained on ultrahigh-resolution CT scans appears useful for assessing coronary artery disease, according to a study published February 10 in Radiology.
The model is a commercially available image reconstruction algorithm that outperformed standard hybrid iterative reconstruction for assessing coronary stenosis in 204 patients who underwent coronary CT angiography (CCTA), noted lead author Limiao Zou, of Peking Union Medical College Hospital in Beijing, China, and colleagues.
“Super-resolution deep learning reconstruction (SR-DLR) is a novel image reconstruction technique developed for coronary CT angiography that offers higher spatial resolution compared with conventional hybrid iterative reconstruction,” the group wrote.
Accurate stenosis assessment with CCTA remains challenging, mainly due to its limited spatial resolution, and advanced image reconstruction methods have attracted interest, the authors explained. To that end, Canon Medical Systems developed its Precise IQ Engine (PIQE) super-resolution deep learning reconstruction technology, which was trained using data acquired with an ultrahigh-resolution CT scanner and is installed on its advanced CT systems.
Previous studies have shown that SR-DLR is superior to conventional iterative reconstruction methods in terms of noise characteristics, spatial resolution, and plaque detectability. However, evidence that supports the application of SR-DLR in stenosis evaluation remains scarce, the authors noted.
To bridge the gap, the researchers tested the performance of SR-DLR versus hybrid iterative reconstruction (HIR) in assessing coronary stenosis, using invasive coronary angiography as the reference standard. They further explored the potential impact of the algorithm on patient-level Coronary Artery Disease Reporting and Data System (CAD-RADS) classification. CAD-RADS is the standardized reporting framework for CCTA.
The study included 204 individuals (mean age, 64.3 years old; 137 male) with 605 plaques (175 calcified, 140 noncalcified, 290 mixed) who underwent clinically indicated CCTA (Aquilion One/Genesis Edition, Canon Medical Systems) and invasive coronary angiography at 10 hospitals across China between September 2023 and November 2024.
Two radiologists, one with four years and one with eight years of clinical experience in cardiac radiology, analyzed the HIR images and SR-DLR images separately for the presence and severity of plaque, separated by a two-week washout period.
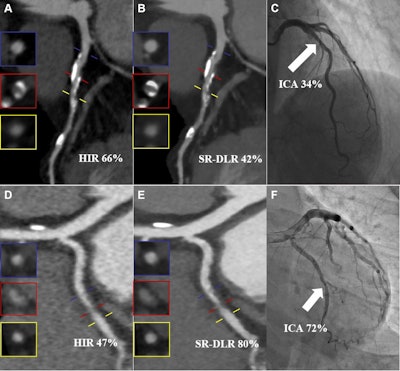
 Images from two representative cases. (A-C) Images in an 82-year-old man with a calcified plaque in the proximal segment of the left anterior descending artery. (A, B) Curved planar reconstruction images from CCTA with (A) hybrid iterative reconstruction (HIR) and (B) super-resolution deep learning reconstruction (SR-DLR) show that the measured PDS was 66% for the HIR image and 42% for the SR-DLR image. (C) Quantitative analysis of the invasive coronary angiography (ICA) image (reference standard) revealed a PDS of 34% (arrow). (D-F) Images in a 37-year-old woman with a noncalcified plaque in the middle segment of the left circumflex artery. (D, E) Curved planar reconstruction images from CCTA with (D) HIR and (E) SR-DLR show that the measured PDS was 47% for the HIR image and 80% for the SR-DLR image. (F) Quantitative analysis of the ICA image revealed a PDS of 72% (arrow). Blue, red, and yellow lines in A, B, D, and E represent the proximal reference point, stenosed lesion, and distal reference point, respectively, and the insets show the corresponding cross-sectional images.RSNA
Images from two representative cases. (A-C) Images in an 82-year-old man with a calcified plaque in the proximal segment of the left anterior descending artery. (A, B) Curved planar reconstruction images from CCTA with (A) hybrid iterative reconstruction (HIR) and (B) super-resolution deep learning reconstruction (SR-DLR) show that the measured PDS was 66% for the HIR image and 42% for the SR-DLR image. (C) Quantitative analysis of the invasive coronary angiography (ICA) image (reference standard) revealed a PDS of 34% (arrow). (D-F) Images in a 37-year-old woman with a noncalcified plaque in the middle segment of the left circumflex artery. (D, E) Curved planar reconstruction images from CCTA with (D) HIR and (E) SR-DLR show that the measured PDS was 47% for the HIR image and 80% for the SR-DLR image. (F) Quantitative analysis of the ICA image revealed a PDS of 72% (arrow). Blue, red, and yellow lines in A, B, D, and E represent the proximal reference point, stenosed lesion, and distal reference point, respectively, and the insets show the corresponding cross-sectional images.RSNA
Key results of the comparison included the following:
The median percentage diameter stenosis for calcified plaques (n = 175) was lower with SR-DLR than with HIR (58% vs. 63%; p
SR-DLR led to 41 of 204 (20%) individuals being assigned a different CAD-RADS category, with 25 downgraded and 16 upgraded.
SR-DLR outperformed HIR in detecting significant stenosis (50% or greater stenosis), with ICA as the reference standard, at both the lesion level (AUC, 0.97 vs. 0.9; p
“SR-DLR outperformed HIR for coronary stenosis assessment,” the researchers wrote.
The authors noted limitations, namely that because the image reconstruction algorithms were from a single vendor, it is unclear to what extent the findings can be generalized to other reconstruction algorithms. Moreover, they wrote that a newer version of the SR-DLR algorithm than was used in this research has been introduced, which will likely be used in future work.
“Further studies are warranted to investigate the impact of CAD-RADS reclassification with SR-DLR on downstream disease management and patient outcomes,” the authors concluded.
The full study is available here.
Whether you are a professional looking for a new job or a representative of an organization who needs workforce solutions - we are here to help.